Silicone breast implants, with or without mastopexy (breast uplift) in the second stage. The second stage timing can be between 6-12 months following the first operation, however, it is variable between patients.

Breast Asymmetry & Mastopexy: What to Expect After Surgery
Overview of Breast Asymmetry & Surgical Correction
Breast asymmetry is a common condition that affects both men and women, though it is more noticeable in females due to differences in breast size, shape, or position. In most cases, breast asymmetry is congenital, meaning it has been present since birth. While minor asymmetry is natural and often does not require medical intervention, some individuals may seek cosmetic surgery due to discomfort, difficulty finding well-fitting clothing, or self-consciousness.
Surgical Options for Breast Asymmetry
Breast asymmetry correction varies based on patient goals and degree of asymmetry. Common procedures include:
1️ Breast Reduction – Reducing the larger breast to match the smaller one. This is more popular among women over 30 years old, especially those who have had children.
2️ Breast Augmentation – Enhancing the smaller breast with an implant or fat transfer for a balanced look.
3️ Mastopexy (Breast Lift) – Lifting one or both breasts to improve symmetry and shape.
4️ Two-Stage Surgery – Involves using expandable breast implants, with gradual size adjustments over time. This is often preferred for younger patients (ages 21-23) whose breasts are still developing.
5️ Hybrid Approach – Combining fat transfer, implants, and mastopexy for optimal results.
A consultation with a board-certified plastic surgeon is essential to determine the best approach for achieving natural, long-lasting symmetry.
What to Expect After Breast Surgery
Hospital Stay & Immediate Recovery
✔ Anaesthesia: Surgery is performed under general anaesthesia.
✔ Overnight Stay: Most patients stay in the hospital for one night for monitoring.
✔ Surgical Drains: Small drainage tubes may be used to remove excess fluid, reducing swelling and promoting healing.
Incisions & Scarring
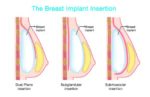
- Incisions depend on the surgical technique and may include:
🔹 Under the breast (inframammary fold)
🔹 Lollipop pattern (vertical incision around the areola and down the breast)
🔹 Anchor-shaped incision (for extensive reshaping) - 🔹Dissolvable stitches are trimmed after 10-12 days.
Post-Surgical Care
✔ Dressing Removal: Dressings are removed after 10-12 days.
✔ Support Bra: A non-wired support bra is recommended for 4-6 weeks to aid healing.
✔ Pain Management:
- Local anaesthetics are used during surgery for pain control.
- Personalized pain relief plans are provided post-surgery.
✔ Swelling & Bruising: Common but subsides within a few weeks.
Fat Transfer & Tissue Expansion Recovery
For patients undergoing fat transfer or tissue expansion, additional steps may include:
✔ Tissue Expansion: Injections of sterile saline solution are performed over time to gradually inflate the breast to the desired size.
✔ Liposuction Garment: Worn for 4-6 weeks to support fat transfer healing.
Returning to Normal Activities
✔ Light activities: Resume within 1-2 weeks.
✔ Full recovery: Expected within 3-4 weeks.
✔ Exercise & Heavy Lifting: Avoid for at least 4-6 weeks.
Psychological Benefits of Breast Asymmetry Surgery
Beyond physical improvements, breast asymmetry correction can significantly boost self-esteem and body confidence. For younger patients, especially teenagers, correcting asymmetry can reduce peer pressure-related stress and improve overall mental well-being.
Final Thoughts
Breast asymmetry correction is a highly personalized procedure, and no two cases are identical. The goal is not perfect symmetry but a natural, proportionate, and aesthetically pleasing result. As a consultant plastic surgeon with nearly 20 years of experience, I have found that the most rewarding aspect of this surgery is seeing patients regain their confidence and embrace their new appearance.
References
- American Society of Plastic Surgeons (ASPS). “Breast Asymmetry: Causes & Surgical Correction.” https://www.plasticsurgery.org
- Mayo Clinic. “Breast Lift and Augmentation: What to Expect.” https://www.mayoclinic.org
- Cleveland Clinic. “Breast Reduction and Reconstruction Procedures.” https://my.clevelandclinic.org